Why Choose Endovascular Treatment For Diabetic Foot?
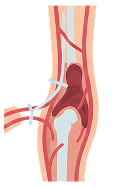
Endovascular treatment for diabetic foot improves blood flow, supports wound healing, and reduces amputation risk without open surgery.
Non‑Surgical
No open incisions; most patients avoid general anaesthesia.

Limb‑Salvage Focused
Revascularization helps healing and lowers major amputation risk.

Faster Recovery
Shorter hospital stay and quicker return to daily activities.

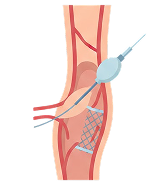
Tailored To Each Artery
Angioplasty, stents, and other tech chosen per disease pattern.